There are over 30 methods described for the correction of epicanthus. Some are more complicated than the others, however, the results of the complicated ones are by mean superior than the simpler ones. In addition, surgery on the inner canthal region is prone to skin contracture and scarring and therefore a method that combines the least number of cutting and cut near the lid margin is preferred.
Some of the epicanthoplasty described are shown below (from Asian Facial Cosmetic Surgery).

Blair method.

Converse method.

Arlt method.

Hiraga method.

Rogeman mthod.

V-W advancement method.
W-plasty method.

Y-V method.

Mustarde method.

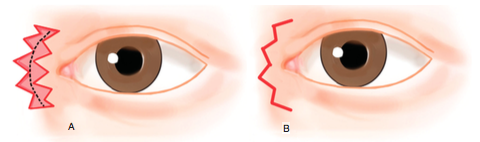
Park Z-plasty method.

Correction of type IV epicanthal folds in blepharophimosis. The picture on the left
was done with Y-V method showing minimal scarring whereas the one shown on
the right was corrected with Mustarde method showing significant skin
contracture and scarring. Pictures taken from an article discussing
the various methods of epicanthoplasty.
My preferred methods for type II and type III epicanthal folds are Park-Z plasty and skin redraping methods. The later will be described in the next blog.

Type III epicanthal fold corrected with Park-Z epicanthoplasty.

































