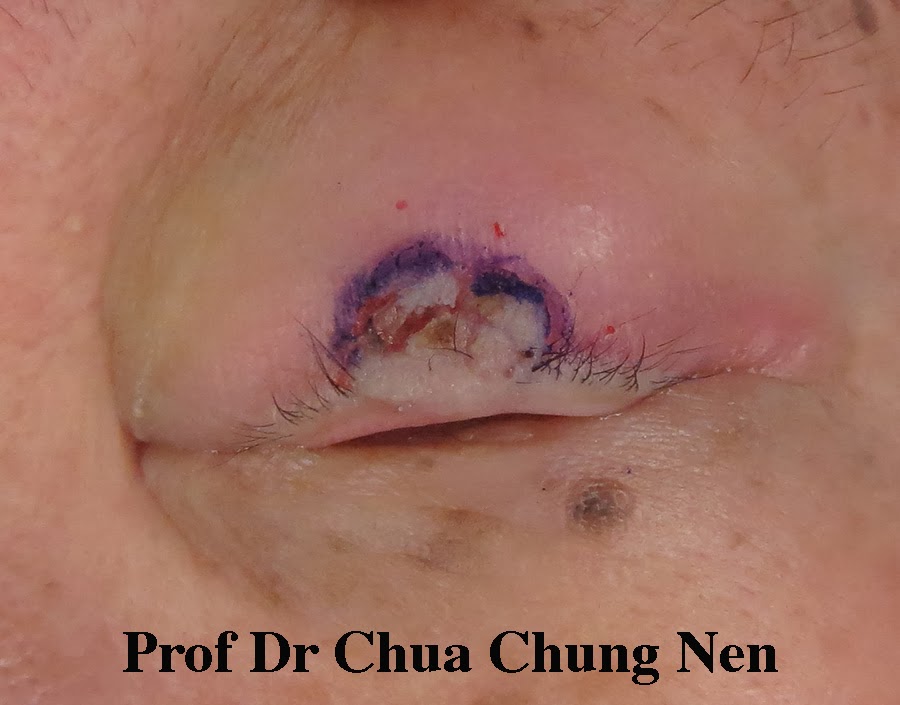
Malignant (cancerous) eyelid tumour is less common in Malaysia than in Western countries because the additional melanin in the skin of the locals protect them against the cancer-causing effect of ultraviolet light. Nevertheless, basal cell carcinoma remains the most common eyelid tumour seen in my oculoplastic clinic. This lesion typically affect people who have chronic sun exposure such as labourers. This 50 year-old man presented with a mass in the right upper eyelid. The lesion first appeared 9 months earlier but grew rapidly along the upper eyelid margin affecting his vision. It also bled easily. Rapid growth and bleeding are two signs suggesting the lesion was a canceroud growth. A biopsy confirmed it was a basal cell carcinoma.

A growth along the right medial 2/3 of the right upper eyelid.
The main objective of treating any cancerous skin lesion is to excise the lesion completely. In this patient, one is faced with the options of either excising the skin tumor alone or take with it 2/3 of the upper eyelid. With the first option, one only need to replace the lost skin but risk leaving behind some tumour; with the second option one can be more certain all tumour is removed but this would leave a big gap needing a bigger reconstruction with longer recovery time and less aesthetic result. In this patient, the tumour invaded only the front of the eyelid with good clear lid margin ( picture b) so I opted for skin excision alone.

Excision of the lesion followed by reconstruction using forehead skin.
The excised lesion was sent for histopathology and after the area was tumour free the forehead skin was used to cover the defect.

Result at one week (pictures a with eyes open and closed)
and two week (b) postoperative.
The patient was able to open his eye at one week and by two weeks the scars were much improved with steroid ointment, sunscreen and sunglasses. He was unable to return for regular visit as he lived 5-hour drive away. He was advised to return in three-month time to check for any recurrence.