With age, the upper eyelid loosens and hangs over the double eyelids and if severe over the eyes giving patients a tired look. Upper blepharoplasty in which the excess skin is excised with or without simultaneous removal of the fat and muscles is a time-tested technique. However, there are some side effects associated with this technique. First, when too much is excised, the thicker upper eyelid will be sutured to the thinner eyelid at or near the junction of the double eyelids. This gives rise to an overhanging appearance (see Figure 1). Second, the removal of excess skin usually extends beyond the double eyelids which gives additional line on the sides of the eyes which may take sometimes to fade. One way of addressing this problem is to use infrabrow excision in selected patients.
Figure 1. A patient who had had upper blepharoplasty.
Note the overhanging thick skin (red arrows) over the skin
creases (double eyelids) and the scars on the temporal
side of the skin creases (black arrows)
This patient came for an eyelid consultation with the desire to lift her upper eyelids so that she looked less tired. She stressed that she did not want any extra lines beyond her double eyelids or the double eyelids to be higher than her existing ones. With upper blepharoplasty, this request could not be met (Fiture 2). However, her eyebrows were high and the excess skin was moderate making her an ideal candidate for infrabrow excision. After discussing the pros and cons of the procedure (the cons being additional scar below the eyebrows, change in shape of the eyebrows and lower eyebrows position), the patient opted for the procedure.
Figure 2. The amount of skin that needs to be excised (red area)
if upper blepharoplasty were performed in this patient.
Figure 3. Removing the skin below the eyebrow will lift
the skin over the eyes and the skin creases.
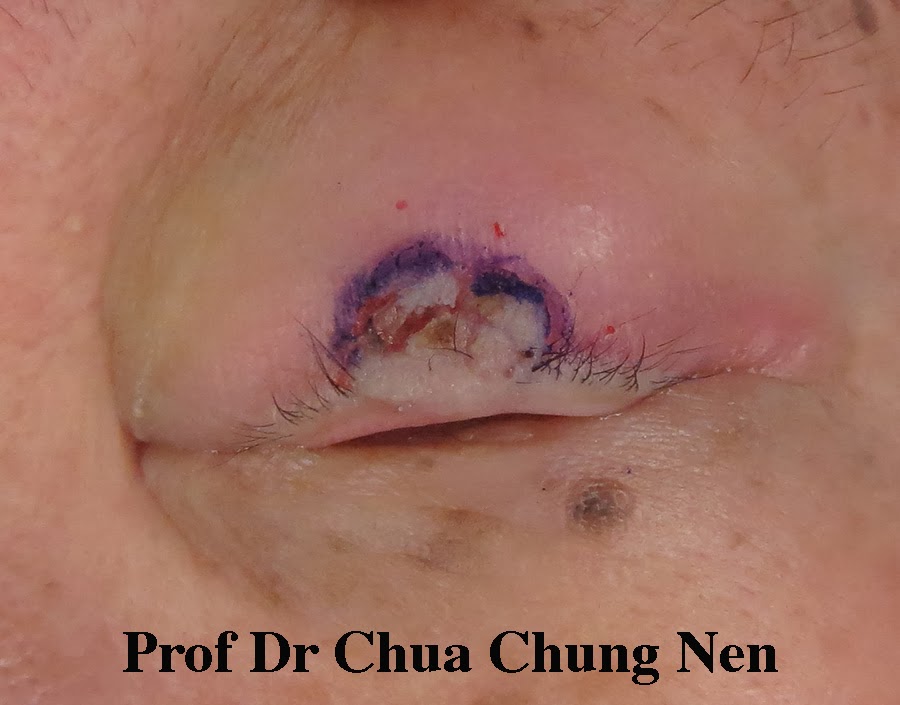
Figure 4. Steps in infrabrow excision. a. The amount of skin to be
excised is marked close to the inferior eyebrows; b. The skin is excised;
c. The excised area should include both the skin and the orbicualris
oculi (the muscle that closes the eyelid); d. The muscle is closed first
with absorbable suture in this case 4/0 vicryl; e. The skin is closed with
5/0 praline and f. At the end of the surgery, the skins are lifted off
the eyes and skin creases (double eyelids).
Infrabrow is ideal for patients without too much loose skin and who can camouflage the scars with make-up or brow embroidery. Therefore, the procedure is performed almost exclusively in females.