This man had had injection to his upper lid in a beauty saloon with an
unknown filler resulting in upper eyelid swellings and occlusion of his visual fields. Examination revealed severe puffiness and hardness of the skin. Hyalase (enzyme to dissolve hyaluronic acid) was injected but the swelling failed to resolve suggesting some sort of permanent filler such as silicone might have been given.
He underwent upper blepharoplasty with removal of the skin, fat and repositioning of the lacrimal glands.
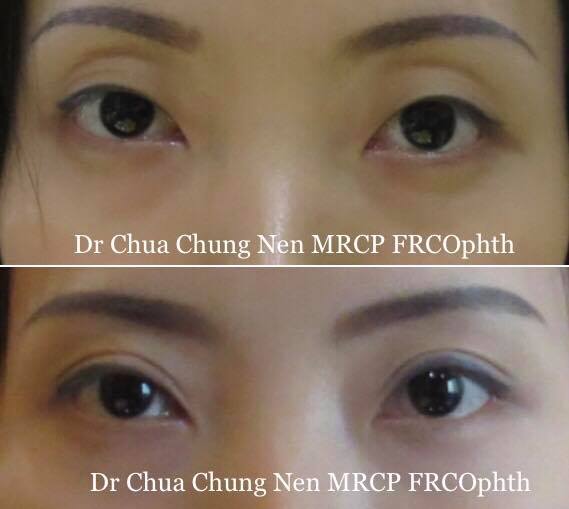
Severe upper eyelid swelling after filler injection,
right lid more puffy than the left.
Proposed height of the skin crease was shown to the patient.
Black arrows shows prominent puffiness of the lateral upper
eyelids indicating there may also be lacrimal gland prolapse.
The skin to be excised was marked and the skin crease was set
The marked area was incised.
The under surface of the excised eyelid showed the filler
as shinny substances (arrowed).
The orbital septum was removed to show the fat.
The lacrimal gland (1) and levator aponeurosis (muscle that
open the eye, 2) were found below the fatty tissue.
The fat that formed part of the upper lid swelling was excised.
The lacrimal gland contributed to the lateral puffiness. Removal
is not recommended as this may cause dry eye.
Instead the lacrimal gland is repositioned using 5/0 ethilon
to the orbital roof.
The lateral puffiness was abolished after lacrimal repositioning.
At the end of the surgery.