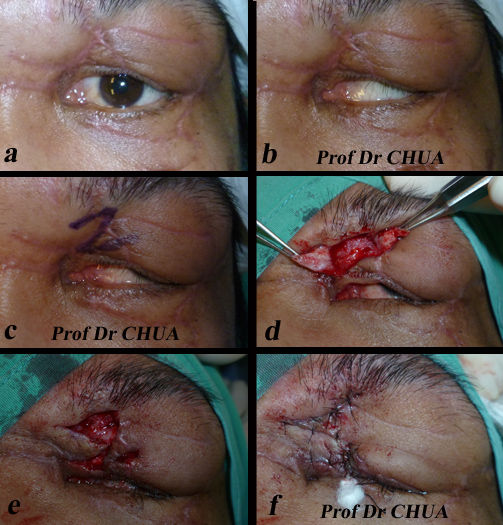
This patient had lower lid blepharoplasty in a beauty saloon two year ago. She complains of dryness of the eyes and rounding of the lower eyelid contour. Examination shows the lower eyelid is tight from excessive skin removal. To restore the normal of the appearance of the eyelid, the skin needs to be replaced. However, the use of skin graft would not aesthetically satisfactory. I recruit the skin by performing disinsertion of the orbiculomalar ligament (see diagram below) and lift the lower eyelid skin by using orbicularis flap (see diagram below) to correct the roundings.

Tightenss of the lower lid and rounding
of the lower lid contours.

Disinsertion of the orbiculomalar ligament.

Disinsertion of the orbiculomalar ligament to recruit
the skin and also to lift the lower lid.

Orbicularis flap is sutured to the orbital periosteum
to lift the lower eyelid.

The picture below was taken at one week after the operation
showing improvement of the retraction
and lower lid contour roundings.








































{kind=link}
{kind=link}